
Hypertension – CEN Emergency Nursing Review 🏥🩺
In the ED, hypertension is either a number (common and often not emergent) or a time-sensitive crisis causing organ injury.
CEN questions love testing whether you can separate asymptomatic elevated BP from hypertensive emergency and choose the correct priorities. 🎯🚑
Fast Jump 🧭
Why this matters •
Anatomy •
Physiology •
Pathophysiology •
ED presentation •
CEN pearls •
Assessment •
Interventions •
Diagnostics •
Complications •
Exam traps •
Rapid review
“Turn Phone Sideways to Take the (10) Question Exam.”
2️⃣ Why This Matters in the Emergency Department 🏥
ED danger = BP + end-organ injury 🚨
- Hypertension can cause acute injury to the brain, heart, aorta, kidneys, and eyes. 🧠🫀🩸🫘👁️
- Hypertensive emergency requires rapid recognition and controlled BP reduction with IV meds (usually ICU-level). 🚑
- Most ED hypertension is asymptomatic elevated BP—treating the number aggressively can cause stroke, MI, syncope from hypoperfusion. ⚠️
- CEN questions test: Do you treat the BP, or the patient? ✅
How it commonly presents in triage 🧾
- Incidental: “Here for ankle pain” with BP 190/110 but no symptoms. 🦶
- Stress/pain/anxiety: elevated BP improves after analgesia, anxiolysis, rest, repeat measurement. 😖
- Emergency symptoms: chest pain, neuro deficits, severe dyspnea, severe headache/vision changes, altered mental status, pregnancy complications. 🚨
3️⃣ Anatomy Review 🧠
The “targets” hypertension injures 🧠🫀🩸🫘👁️
- Arteries/arterioles: high pressure damages endothelium → vasoconstriction, inflammation, thrombosis. 🩸
- Brain: small vessels → hemorrhage/ischemia; swelling → encephalopathy. 🧠
- Heart: coronary demand increases → ischemia/MI; LV hypertrophy → HF. 🫀
- Aorta: high shear stress → dissection risk. 🩸🧨
- Kidneys: glomerular injury → AKI. 🫘
- Eyes: retinal vessel damage → visual changes, papilledema (severe). 👁️
4️⃣ Physiology Review ⚙️
BP basics nurses must know ✅
- BP ≈ CO × SVR (cardiac output × systemic vascular resistance). 🫀🩸
- SVR rises with vasoconstriction (stress, pain, catecholamines, drugs). ⚡
- Autoregulation: brain/kidneys adapt to chronic high BP; dropping BP too fast can cause hypoperfusion. 🧠🫘
- MAP (mean arterial pressure) drives organ perfusion—CEN questions often focus on perfusion, not just systolic numbers. 🎯
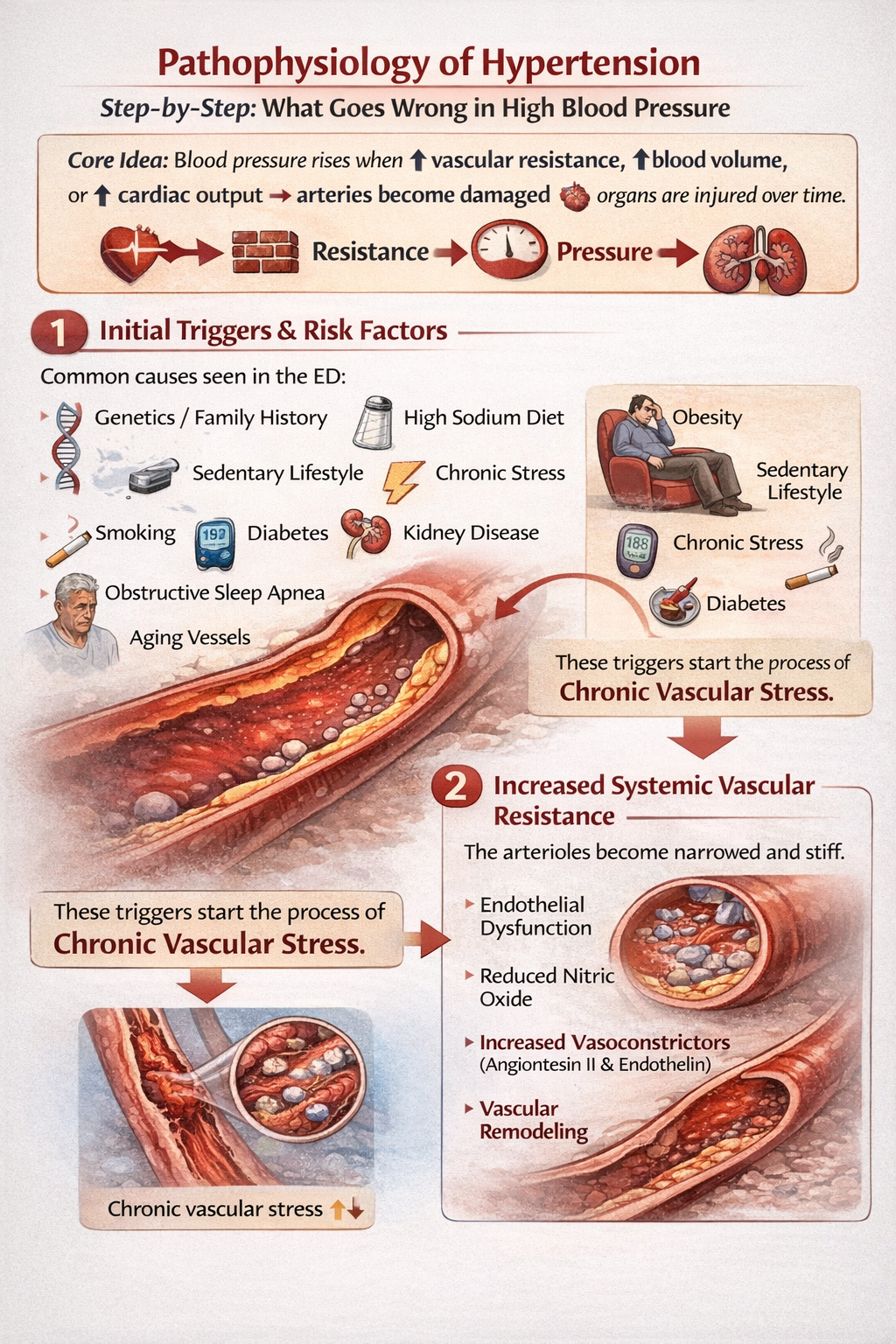
5️⃣ Pathophysiology 🚨
Step-by-step: what goes wrong in hypertensive crisis 🧠
Core idea: a sudden, severe rise in BP overwhelms autoregulation → endothelial injury + vasoconstriction + organ ischemia/bleeding. 🩸⚠️
- Trigger: missed meds, stimulant use (cocaine/amphetamines), renal failure, endocrine causes, pregnancy, pain/anxiety, withdrawal, or acute illness. 💊⚡
- SVR spikes (vasoconstriction) → BP rises further. 🩸⬆️
- Endothelial damage → leaky vessels, platelet activation, microthrombi. 🩸
- Organ injury develops:
- Brain: stroke/ICH/encephalopathy (confusion, seizures). 🧠
- Heart: ACS, acute HF/flash edema. 🫀🫁
- Aorta: dissection. 🧨
- Kidneys: AKI. 🫘
- Eyes: retinal hemorrhages/papilledema. 👁️
6️⃣ Classic Emergency Department Presentation 🚑
Hypertension “types” in the ED (CEN favorite) 🎯
1) Asymptomatic elevated BP 🟢
High BP reading but no end-organ symptoms. Often due to pain, anxiety, missed meds, or chronic HTN.
2) Hypertensive urgency (older term) 🟡
Severe BP elevation with mild symptoms (e.g., headache) but no objective end-organ damage. ED focus = assess, treat contributing factors, adjust meds, close follow-up.
3) Hypertensive emergency 🔴🚨
Severe BP elevation + acute target-organ damage (stroke/ICH, ACS, pulmonary edema, aortic dissection, AKI, eclampsia, etc.). Requires IV meds + controlled reduction + critical care.
What triage nurses might notice 🧾
- Neuro: weakness, slurred speech, confusion, seizure, “worst headache.” 🧠
- Cardiac: chest pressure, diaphoresis, new ischemic EKG changes. 🫀
- Resp: severe SOB, crackles, pink frothy sputum (flash edema). 🫁
- Aorta: ripping/tearing chest/back pain, pulse/BP differential, syncope. 🧨
- Pregnancy: headache, RUQ/epigastric pain, vision changes, edema, seizures. 🤰🚨
7️⃣ High-Yield CEN Exam Pearls 🎯
The “CEN decision point” ✅
Numbers alone do NOT define emergency. The presence of end-organ damage does. 🎯
- Repeat BP correctly: right cuff size, seated/rested, arm at heart level, recheck manually if needed. 🩺
- Don’t drop BP too fast in chronic HTN—risk cerebral/renal hypoperfusion. 🧠🫘
- Flash pulmonary edema + severe HTN: high yield for early NIV + IV vasodilator strategy per provider. 🫁📉
- Aortic dissection: goal is to reduce shear stress—control HR/BP rapidly per protocol (often beta-blockade first). 🧨
- Pregnancy (preeclampsia/eclampsia): seizure prevention/management and BP control are critical; magnesium is a key medication. 🤰💊
8️⃣ Emergency Nursing Assessment 🩺
What to assess (history + exam + red flags) 🧾
Key history questions 🎯
- Baseline BP? Known HTN? Current meds and missed doses? 💊
- Symptoms of organ injury: chest pain, dyspnea, neuro changes, vision changes, decreased urine output. 🧠🫀🫁👁️🫘
- Drug exposure: cocaine/amphetamines, decongestants, MAOIs, steroids, withdrawal. ⚡
- Pregnancy status and gestational age; headache/RUQ pain/vision changes. 🤰
Focused exam 🩺
- Neuro assessment (FAST, pupils, mental status). 🧠
- Heart/lungs: ischemia signs, crackles/pulmonary edema. 🫀🫁
- Perfusion: skin temp, pulses; compare BP in both arms if dissection suspected. 🩸
- Fundoscopic/vision complaint cues (severe cases). 👁️
Immediate red flags 🚨: focal neuro deficit, altered mental status, seizure, chest pain with ischemic EKG, severe dyspnea/pulmonary edema, tearing chest/back pain, pregnancy + neuro symptoms/RUQ pain, hypotension in suspected dissection. 🧠🫀🫁🧨🤰
9️⃣ Priority Interventions 🚑
ED nursing priorities (do this first + why) 🏥
First action: confirm BP and assess symptoms. Treat pain/anxiety, repeat BP appropriately, and rapidly screen for end-organ injury. Rationale: most elevated BP is not an emergency, but emergencies must be caught early. 🩺✅
If asymptomatic elevated BP 🟢
- Recheck BP, address pain/anxiety, review home meds, ensure follow-up. 🧾
- Avoid rapid IV BP drops unless directed for a true emergency. ⚠️
If hypertensive emergency 🔴🚨
- Continuous cardiac monitoring, frequent BP checks (often q5–15 min per protocol), 2 IVs if unstable. ⚡🩺
- Prepare for IV antihypertensive infusion/bolus meds per provider; titrate carefully and reassess neuro status/perfusion. 💊
- Support ABCs: O2/NIV for pulmonary edema, treat dysrhythmias/ACS pathways as indicated. 🫁🫀
- Escalate early (ICU/CT/echo) based on suspected organ injury. 🚑
Key nursing principle 🎯: BP reduction should be controlled. A rapid, large drop can reduce cerebral perfusion and worsen outcomes—especially in chronic HTN. 🧠⚠️
🔟 Diagnostic Tests 🔬
Tests depend on suspected organ injury 🎯
- EKG + troponin: ischemia/ACS, LVH strain. ⚡🧪
- CXR: pulmonary edema, widened mediastinum clues (dissection context). 🩻
- CMP: creatinine/electrolytes for renal injury and medication safety. 🫘🧪
- Urinalysis: protein/hematuria (renal involvement; pregnancy workup). 🧪
- Neuro imaging (CT head) if stroke/ICH symptoms. 🧠
- CT angiography if aortic dissection suspected. 🧨
- Pregnancy labs (per protocol): platelets, LFTs, urine protein, etc. 🤰
- POCUS: LV function, B-lines (edema), aortic root clues (context-dependent). 🔬
11️⃣ Complications ⚠️
When BP causes damage (or treatment causes harm) 🚨
- Stroke/ICH, hypertensive encephalopathy, seizures. 🧠
- ACS/MI, acute HF/flash pulmonary edema. 🫀🫁
- Aortic dissection. 🧨
- AKI. 🫘
- Retinal hemorrhage/vision loss. 👁️
- Iatrogenic hypoperfusion if BP is lowered too quickly. ⚠️
12️⃣ CEN Exam Traps 🚨
Most common CEN mistakes 🎯
- Trap: Treating asymptomatic high BP with aggressive IV meds.
Fix: Assess for end-organ damage first; recheck BP properly; address pain/anxiety; ensure follow-up. ✅ - Trap: Calling headache alone a hypertensive emergency.
Fix: Look for objective neuro findings, AMS, papilledema, seizure, ICH signs. 🧠 - Trap: Missing aortic dissection.
Fix: Sudden tearing pain + neuro deficits/pulse deficit/BP differential = emergency until proven otherwise. 🧨 - Trap: Dropping BP too fast in chronic HTN.
Fix: Controlled reduction with frequent reassessment—protect cerebral/renal perfusion. 🧠🫘 - Trap: Missing pregnancy-related hypertensive crisis.
Fix: Headache + vision changes + RUQ pain + pregnancy/postpartum = treat as high risk. 🤰🚨
13️⃣ Rapid Review Summary 🧠
One-minute HTN recap 🏥✅
- HTN emergency = BP + acute end-organ damage (brain, heart, aorta, kidneys, eyes). 🧠🫀🧨🫘👁️
- Most ED HTN is not emergent — confirm BP, treat pain/anxiety, review meds, arrange follow-up. 🩺
- Do NOT drop BP too fast in chronic HTN — risk hypoperfusion stroke/AKI. ⚠️
- Flash pulmonary edema + severe HTN = NIV + afterload reduction strategy per provider. 🫁📉
- Aortic dissection pattern: sudden tearing chest/back pain + pulse/BP differential → immediate escalation. 🧨
- Pregnancy red flags: headache/vision changes/RUQ pain/seizure → treat urgently. 🤰🚨
Study tip 🧠: On CEN questions, if BP is high, immediately ask: “Where is the organ injury?” If you can’t find it, the priority is usually repeat BP correctly + symptom control + safe disposition/follow-up — not IV drips. 🎯🏥


Learn Emergency Medicine From Someone Who Has Lived It
For more than 35 years in emergency medicine, Jeffery Bratcher has worked in environments where seconds matter, prioritization saves lives, and clinical judgment must be immediate.
The CEN® exam tests that exact type of thinking. Elite CEN Prep was built to train emergency nurses to recognize patterns, prioritize care, and answer exam questions the same way experienced ER clinicians think.
This is not memorization. This is clinical reasoning training for emergency nurses.
Train Your Brain to Think Like a Certified Emergency Nurse
The CEN® exam costs nearly $380–$450.
Elite CEN Prep gives you a complete certification system including
2,100+ questions with rationales, 6 full-length exam simulations, and deep-dive training videos.
The full price of Elite CEN Prep will soon increase to $97 as new training modules and content are added.
Secure your access now and lock in the $67 founding price before the increase.
🔥 Start Elite CEN Prep Now ($67)
📚 Purchase the Timed CEN Simulation Exam (150 Questions) $15 Dollars