
Heart Failure – CEN Emergency Nursing Review 🏥🫀
Heart failure is one of the most common, high-risk ED presentations. It can look like “just shortness of breath,”
but it can rapidly become respiratory failure, cardiogenic shock, or a dysrhythmia-driven arrest.
For the CEN exam, success is about recognizing patterns fast, prioritizing the right interventions, and avoiding classic traps. 🚑⚡
Fast Jump 🧭
Why this matters •
Anatomy •
Physiology •
Pathophysiology •
ED presentation •
CEN pearls •
Assessment •
Interventions •
Diagnostics •
Complications •
Exam traps •
Rapid review
2️⃣ Why This Matters in the Emergency Department 🏥
Why ED nurses must recognize heart failure FAST 🚨
- Heart failure can deteriorate into flash pulmonary edema → hypoxia → respiratory failure. 🫁📉
- It can be driven by reversible triggers (ACS, dysrhythmias, hypertension, infection, noncompliance). Finding the cause changes everything. 🎯
- Missed HF can be mistaken for COPD/asthma, pneumonia, or PE → delays in diuresis/vasodilation/ventilation support. 🧠
- Bad outcomes include need for intubation, cardiogenic shock, renal failure, and death. ⚠️
- In triage it often presents as: “SOB,” “can’t lie flat,” “swelling,” “weight gain,” “cough,” “fatigue”. 🧾
“Turn Phone Sideways to Take the (10) Question Exam.”
The ED nurse mindset 🧠
- First question: Is the patient oxygenating and ventilating? (work of breathing matters). 🫁
- Second question: Warm & wet vs cold & wet? (perfusion + congestion). 🩸
- Third question: What is the trigger? (ACS, AF RVR, HTN crisis, infection, meds/diet). 🎯
3️⃣ Anatomy Review 🧠
Structures you must “see” in your head 🫀
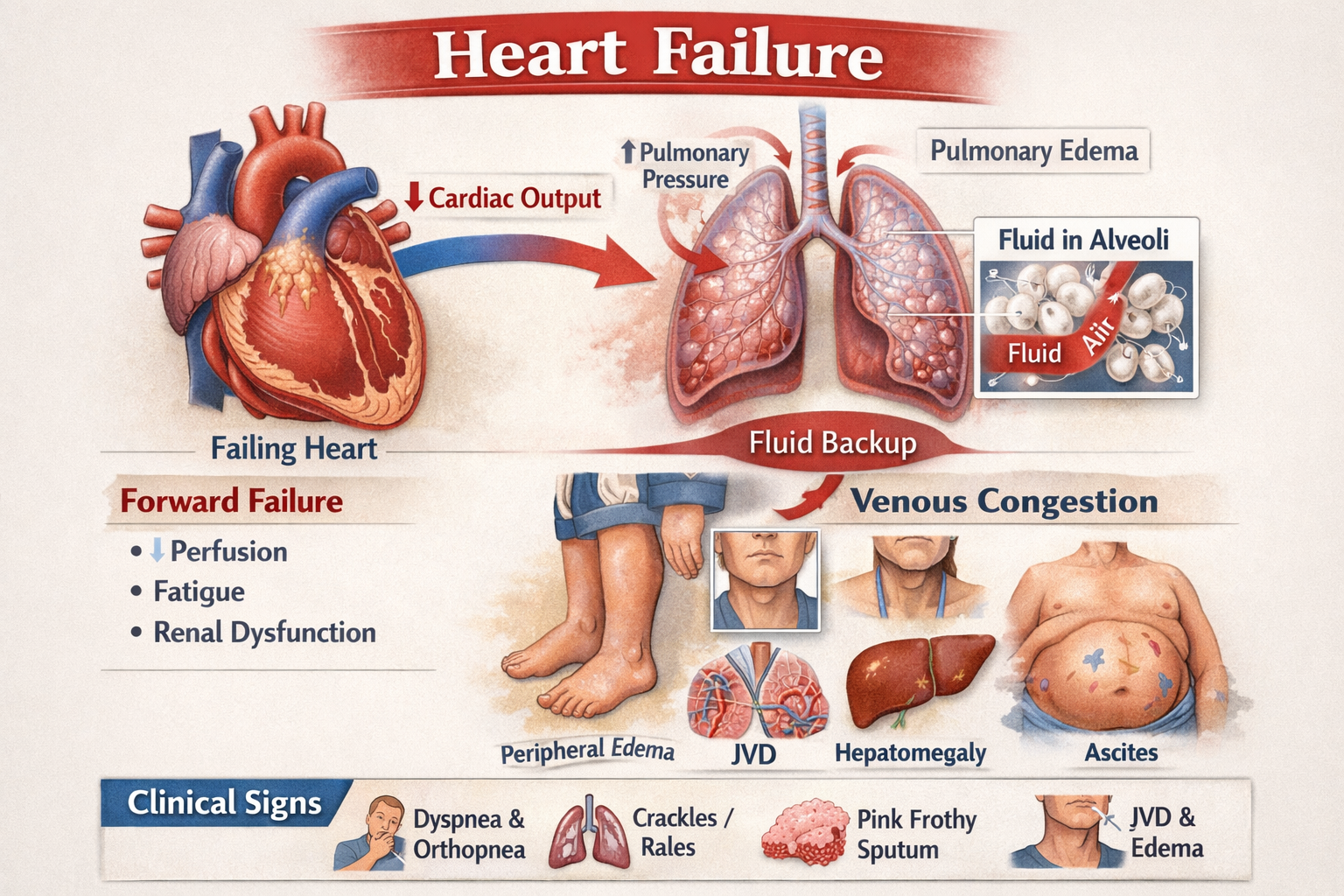
- Left ventricle (LV): main pump to body; LV failure → pulmonary congestion/edema. 🫁
- Right ventricle (RV): pumps to lungs; RV failure → systemic congestion (JVD, edema, hepatomegaly). ⬆️🦶
- Valves (mitral/aortic/tricuspid): regurg/stenosis increases workload and worsens HF. 🚪
- Pulmonary capillaries: fluid backs up here → crackles, hypoxia, pink frothy sputum (severe). 💧
- Kidneys: perfusion + RAAS activation drives sodium/water retention → more volume overload. 🫘
“Turn Phone Sideways to Take the (10) Question Exam.”
4️⃣ Physiology Review ⚙️
What should normally be happening 🧠➡️🫀➡️🩸
- Cardiac output (CO) = heart rate × stroke volume. Enough CO = good perfusion and organ function. 🩸
- Preload = ventricular filling/volume coming in. Too much preload can flood the lungs when the LV is weak. 💧
- Afterload = resistance the heart pumps against (SVR/BP). High afterload (HTN) can trigger flash pulmonary edema. 📈
- Ejection fraction (EF) reflects systolic pumping (HFrEF). Some patients have preserved EF but stiff ventricles (HFpEF). 🫀
- RAAS/SNS help short-term (vasoconstriction + fluid retention) but worsen HF long-term. ⚡🧂
5️⃣ Pathophysiology 🚨
Step-by-step: what goes wrong in heart failure 🧠✅
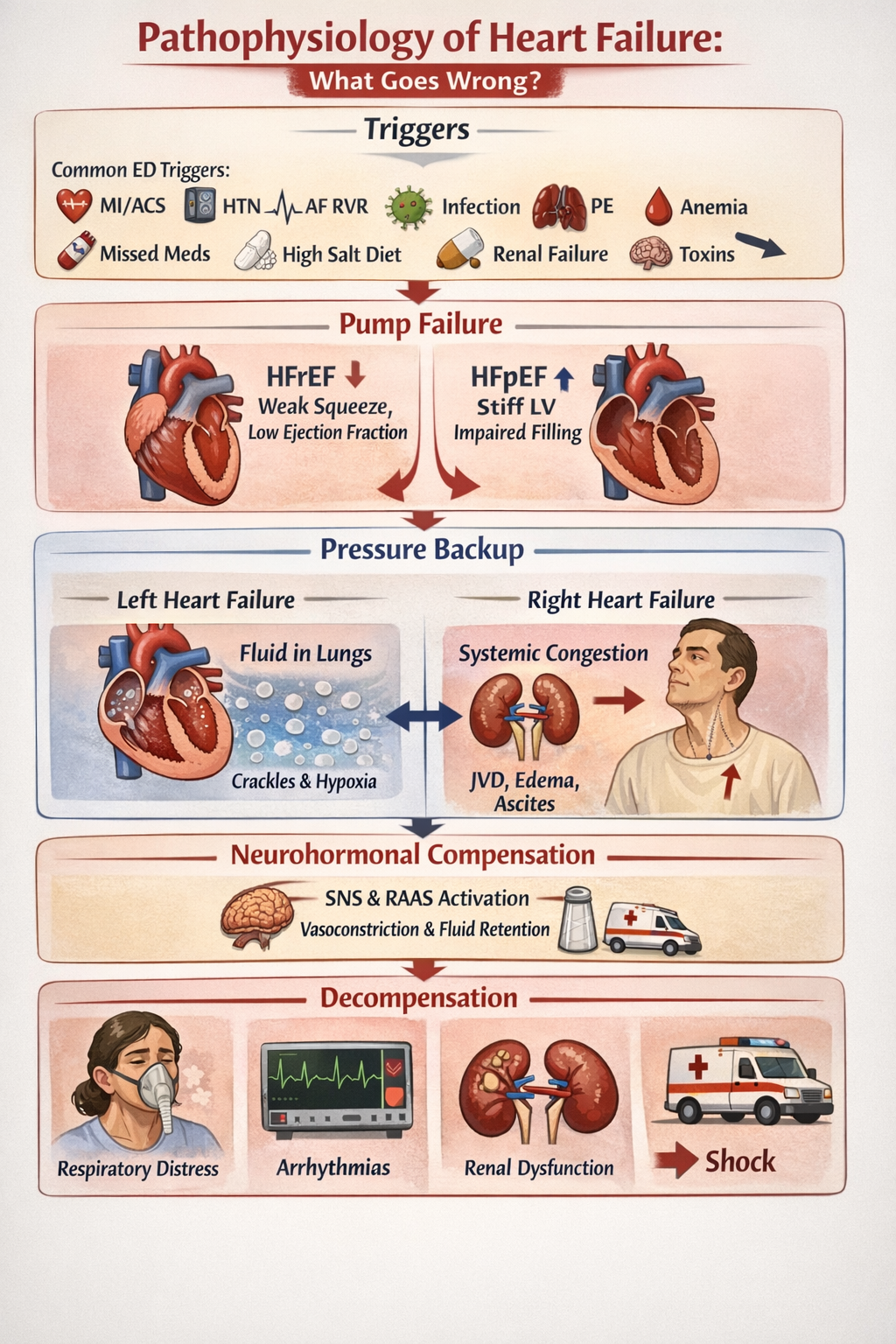
Core idea: the heart can’t pump effectively (or can’t fill effectively) → pressure backs up → fluid shifts into lungs/body + organs get underperfused. 🫀➡️💧➡️📉
- Trigger hits (common ED triggers): ACS/MI, uncontrolled HTN, AF RVR, infection/sepsis, PE, anemia, missed meds, high-salt diet, renal failure, toxins. 🎯
- Pump failure or filling failure:
- HFrEF: weak squeeze → low EF → poor forward flow. 🫀
- HFpEF: stiff LV → high filling pressures even with “normal EF.” 🧱
- Back-up pressure builds behind the failing side:
- LV failure → pulmonary venous congestion → alveolar fluid → crackles/hypoxia. 🫁💧
- RV failure → systemic venous congestion → JVD, edema, ascites. ⬆️🦶
- Neurohormonal compensation (SNS/RAAS) causes vasoconstriction + fluid retention → temporarily supports BP but worsens congestion. ⚡🧂
- Decompensation leads to: respiratory distress, dysrhythmias, renal dysfunction, shock. 🚑📉
6️⃣ Classic Emergency Department Presentation 🚑
What you see in triage + primary survey 🏥
- Chief complaints: SOB, orthopnea (can’t lie flat), PND (wakes up gasping), edema, weight gain, fatigue, cough. 🫁🛏️
- Appearance: anxious, tripod, speaking in short phrases, diaphoretic (severe). 😮💨
- Lung sounds: crackles/rales, sometimes wheezes (“cardiac asthma”). 🫁
- Vitals patterns: tachypnea, tachycardia; may be hypertensive (flash edema) or hypotensive (shock). 📈📉
- Other clues: JVD, S3 gallop, peripheral edema, cool/clammy extremities if low perfusion. ⬆️🦶❄️
Flash pulmonary edema pattern 🚨: sudden severe SOB, very high BP, frothy sputum, diffuse crackles, extreme distress. Think: afterload problem + acute fluid shift. 🫁💥
7️⃣ High-Yield CEN Exam Pearls 🎯
Recognize these testable patterns ✅
- Orthopnea + PND are highly suggestive of HF congestion. 🛏️🫁
- S3 gallop = volume overload / decreased ventricular compliance (classic HF finding). 🎧
- BNP/NT-proBNP supports HF (not perfect; interpret with clinical picture). 🧪
- CXR clues: vascular congestion, interstitial edema, cardiomegaly, pleural effusions. 🩻
- POCUS clues: B-lines (pulmonary edema), plethoric IVC, reduced EF (operator dependent). 🔬
- Cold & wet (poor perfusion + congestion) = higher risk; may need ICU-level care. ❄️💧
- AF RVR can cause decompensation; rate control + treating congestion may be key. ⚡
- Hypertensive HF often needs vasodilation + noninvasive ventilation early. 📈🫁
8️⃣ Emergency Nursing Assessment 🩺
What to assess (history + exam + red flags) 🧾
Key history questions 🎯
- Known HF? Last EF? Recent admissions? Baseline weight and oxygen use? 🫀
- Medication adherence (diuretics!), missed doses, recent diet/“salty foods,” fluid intake. 💊🧂
- Chest pain/pressure (ACS), palpitations (AF RVR), fever/cough (infection). 🧠
- Rapid onset vs gradual (flash edema vs slow volume overload). ⏱️
- Renal disease/dialysis schedule missed? 🫘
Focused physical exam 🩺
- Work of breathing: accessory muscles, ability to speak, mental status changes. 🫁
- Lungs: crackles, wheeze, diminished bases (effusions). 🫁
- Perfusion: cool/clammy, cap refill, mentation, urine output trend. 🩸
- JVD, edema, hepatomegaly; look for sacral edema in bedbound patients. ⬆️🦶
Immediate red flags 🚨: SpO2 low despite O2, severe distress, hypotension, altered mental status, chest pain with ischemic EKG changes, sustained VT, pink frothy sputum, rising CO2/respiratory fatigue. 🫁⚡📉
9️⃣ Priority Interventions 🚑
ED priorities (what you do first + why) 🏥
First 5 minutes: Sit up, apply O2 as needed, continuous monitor, obtain IV access, get an EKG, and assess WOB/perfusion. Rationale: HF can crash into respiratory failure or lethal dysrhythmia. 🪑🫁⚡
Airway/Breathing support 🫁
- Noninvasive ventilation (CPAP/BiPAP) early for moderate–severe distress/edema (per protocol). Rationale: recruits alveoli, improves oxygenation, reduces preload/afterload. 🫁✅
- Prepare for intubation if failing NIV, exhausted, or altered. Rationale: respiratory fatigue can lead to arrest. ⚠️
Circulation & hemodynamics 🩸
- Hypertensive acute HF / flash edema: anticipate vasodilators per provider (e.g., nitrates) + NIV. Rationale: reduce afterload, improve forward flow quickly. 📈➡️📉
- Volume overloaded (“wet”): anticipate IV diuretics per provider; monitor urine output. Rationale: removes excess fluid and improves pulmonary congestion. 🚽💧
- Hypotensive / cold & wet: cautious fluids only if truly dry; prepare pressors/inotropes per provider and ICU escalation. Rationale: diuresis/vasodilation can worsen shock if perfusion is failing. 📉🚨
Monitoring & nursing workflow ✅
- Strict I&O; consider external catheter; daily weights if admitted. 🧾
- Frequent lung reassessment after NIV/diuretics/vasodilators. 🫁
- Watch electrolytes (K/Mg) and rhythm changes with diuresis. ⚡🧪
- Treat the trigger: ACS pathway, infection workup, AF RVR management, BP control. 🎯
🔟 Diagnostic Tests 🔬
What to order/expect (and what it tells you) 🧪
- EKG: ischemia, AF RVR, conduction blocks, LVH strain. ⚡
- CXR: cardiomegaly, pulmonary vascular congestion, interstitial/alveolar edema, pleural effusions. 🩻
- BNP/NT-proBNP: supports HF; interpret with age/renal function/obesity. 🧪
- Troponin: assesses for ACS/demand ischemia (common trigger). 🧪
- CBC/CMP: anemia, infection, renal function (diuretic dosing/risks), electrolytes. 🧫🫘
- ABG/VBG (if severe): ventilation status, CO2 retention, acid-base; look for impending fatigue. 🫁
- POCUS: B-lines, IVC size/collapsibility, EF estimate, pleural effusions. 🔬
- Echo (often inpatient/urgent): EF, valve function, wall motion. 🫀
11️⃣ Complications ⚠️
What can go wrong if HF worsens 🚨
- Respiratory failure (worsening pulmonary edema) → intubation. 🫁⚠️
- Cardiogenic shock → hypotension, cool extremities, AMS, low urine output. 📉🧠
- Malignant dysrhythmias (VT/VF), bradyarrhythmias, sudden cardiac death. ⚡
- Renal failure (cardiorenal syndrome). 🫘
- Myocardial ischemia from demand or ACS trigger. 🫀
12️⃣ CEN Exam Traps 🚨
Avoid these common exam mistakes 🎯
- Trap: Treating HF wheeze like asthma with aggressive fluids and repeated bronchodilators only.
Fix: Consider “cardiac asthma” — look for edema, JVD, BNP/CXR clues; support ventilation and manage congestion. 🫁 - Trap: Large IV fluid bolus for tachycardia without assessing volume status.
Fix: HF patients are often “wet”; reassess lungs/IVC/perfusion before fluids. 💧 - Trap: Delaying NIV until after meds “kick in.”
Fix: Early CPAP/BiPAP can rapidly improve oxygenation and reduce work of breathing. ✅ - Trap: Missing the trigger (ACS, AF RVR, HTN crisis, infection).
Fix: HF is often the result — treat the cause while treating symptoms. 🎯 - Trap: Over-diuresis/vasodilation in hypotensive “cold & wet” patients.
Fix: This group may need pressors/inotropes and ICU escalation. 📉🚨
13️⃣ Rapid Review Summary 🧠
One-minute HF recap 🏥✅
- Think HF with SOB + orthopnea/PND + crackles + edema/JVD. 🫁⬆️
- First priorities: sit up, O2, monitor, IV, EKG, assess WOB + perfusion. 🪑🫁⚡
- Early NIV for distress/edema = high yield in ED care. ✅
- Hypertensive flash edema often needs vasodilation + NIV fast. 📈➡️📉
- Diuretics help volume overload; monitor K/Mg + urine output. 💧🧪
- Cold & wet (shock + congestion) = high risk → escalate to ICU, pressors/inotropes per provider. 📉🚨
- Always search for the trigger: ACS, AF RVR, infection, HTN crisis, renal failure, nonadherence. 🎯
Study tip 🧠: On CEN questions, decide if the patient is oxygenating, congested (wet), and/or poorly perfused (cold). Then choose the priority action that fixes the biggest immediate threat: NIV for distress, vasodilation for hypertensive flash edema, or shock management + escalation for cold & wet. 🏥✅


Learn Emergency Medicine From Someone Who Has Lived It
For more than 35 years in emergency medicine, Jeffery Bratcher has worked in environments where seconds matter, prioritization saves lives, and clinical judgment must be immediate.
The CEN® exam tests that exact type of thinking. Elite CEN Prep was built to train emergency nurses to recognize patterns, prioritize care, and answer exam questions the same way experienced ER clinicians think.
This is not memorization. This is clinical reasoning training for emergency nurses.
Train Your Brain to Think Like a Certified Emergency Nurse
The CEN® exam costs nearly $380–$450.
Elite CEN Prep gives you a complete certification system including
2,100+ questions with rationales, 6 full-length exam simulations, and deep-dive training videos.
The full price of Elite CEN Prep will soon increase to $97 as new training modules and content are added.
Secure your access now and lock in the $67 founding price before the increase.
🔥 Start Elite CEN Prep Now ($67)
📚 Take the CEN Simulation (150 Questions)